

The Lancet Global Health Oxygen Commission
Two and half years in the making, The Lancet Global Health Commission on Medical Oxygen Security released its report on 17 February 2025. You can watch the 18 February 2025 official global launch here and read the full Commission report and Comments here and related documents below including:
- Media Statement
- Presentation Deck
- Policy briefs in English, French, Spanish, Russian, Chinese, and Arabic.
- Spotlight briefs:
- Country Case Studies from Bangladesh, India, Malawi, Nigeria, Sweden, and Uganda.
- Video testimonials from Saude Abdullahi (Nigeria), Baby Ahammad’s Family (Bangladesh), Aggrey Aluso (Kenya), Nomawethu Jele (South Africa), Blessi Kumar (India), and Maurine Murenga (Kenya) here.
- Alexander Mandl’s powerful story about long-term dependence on medical oxygen while waiting for a double lung transplant here.
- Don’t miss the podcast interview with The Lancet Global Health editor-in-chief Zoë Mullan and two of the Commission authors, Dr Carina King and Dr Ehsan Rahman, here.
- Report from the Africa launch in Nigeria with Communique here.
- All of the evidence that informed the Commission is now available in the A2O2 Resource Library, hosted by PATH here!
Who led The Lancet Global Health Oxygen Commission?
The Commission was overseen by 18 Commissioners – academic experts representing all regions – and 40 Advisors provided guidance, supported by an Executive Committee including Makerere University (Uganda), icddr,b (Bangladesh), the University of Melbourne/Murdoch Children’s Research Institute (Australia), the Karolinska Institutet (Sweden), and the Every Breath Counts Coalition (USA). The Commission also engaged regularly with a global network of Oxygen Access Collaborators and conducted interviews with patients, caregivers, and clinicians and consultations with governments and industry.
Why did we need a commission?
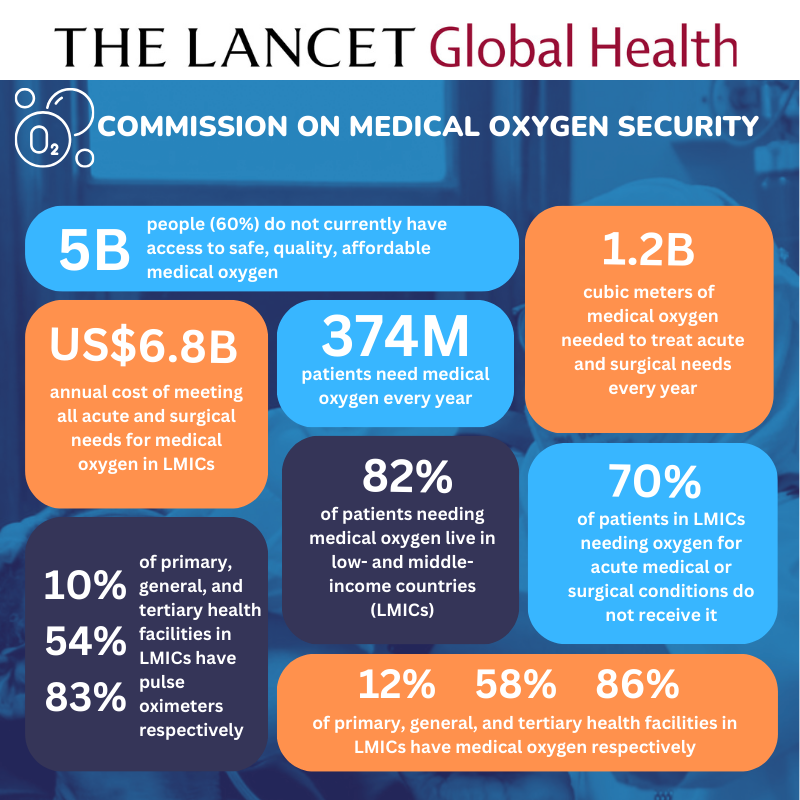
Medical oxygen is an essential medicine with no substitute for the treatment of at least 20 Global Burden of Disease conditions, including HIV/AIDS, TB, malaria, pneumonia, COVID-19, maternal and neonatal disorders, tracheal, bronchus, and lung cancers, anemia, sickle cell disease, heart disease, stroke, COPD, asthma, transport injuries, poisonings, foreign body injuries, self-harm, and interpersonal violence. Together, these conditions caused a massive 40 million deaths in 2021, almost 60% of all human deaths.
Medical oxygen is particularly lifesaving for newborns and children. A recent review found that deaths among hospitalized children fell by 25% when pulse oximetry and oxygen was provided, and that oxygen is as cost-effective as childhood vaccination. But oxygen is often unavailable in health facilities, especially those located in low- and middle-income countries (LMICs). And where it is available, it is often unaffordable leaving the most vulnerable patients without access to a lifesaving medicine.
COVID-19 exposed a tragic gap
Lack of medical oxygen was a defining inequity of the COVID-19 pandemic, with LMICs bearing the brunt of oxygen shortages and related deaths. The pandemic exposed not only a tragic gap in inadequate supplies of medical oxygen and respiratory therapies, but also the trained workforce needed to install, operate, and maintain the lifesaving equipment. The gap had always been there – contributing to a massive burden of death that was largely hidden. When COVID-19 unleashed a new wave of patients needing oxygen, hospitals were unable to meet the demand and the world watched as patients died waiting for oxygen on gurneys in the parking lots of hospitals, in the backseats of cars, and at home waiting for loved ones to return with filled cylinders.
A study of COVID-19 deaths in 64 intensive care units across 10 African countries showed that one in two patients died without receiving medical oxygen, and a study from Peru, which recorded the highest COVID-19 death rate in the world, found that oxygen saturation below 90% on admission was a strong predictor of mortality. The authors concluded that in settings with limited resources, efforts to reduce COVID-19 deaths should focus on early identification of hypoxemia and timely access to oxygen.
Oxygen gaps remain in many countries
Despite the additional oxygen supplies many countries received during the pandemic, including US$1 billion from the ACT-Accelerator Oxygen Emergency Taskforce, access gaps remain. Many governments still do not know how much oxygen their health systems need to meet the needs of patients during routine times, or how much surge capacity will be needed when the next respiratory pandemic strikes. Likewise, global health partners are in the dark about how much, and what kind, of oxygen support different countries need to strengthen their health systems most cost-effectively.
The Lancet Global Health Commission on Medical Oxygen Security is a major effort to change this. Announced in September 2022, the Commission sheds light onto the number of patients needing medical oxygen each year in each region and the cost of meeting that need, how to define and measure oxygen coverage, which oxygen solutions work best in different settings, and how to generate the financing and political will to achieve transformational change. It addresses all levels of care from hospital to home, all age groups from neonates to the elderly, all health conditions where oxygen is a recommended treatment, and all the ways in which access to oxygen can contribute to health system strengthening and pandemic preparedness.
Promising new developments
Governments and global health and development agencies urgently need this information as they pivot from pandemic response to preparing for the next crisis and return to the job of achieving the Sustainable Development Goals. The new Global Oxygen Alliance (GO₂AL), co-chaired by The Global Fund and Unitaid, and the World Health Organization’s Increasing Access to Medical Oxygen Resolution, endorsed by all 194 Member States, are both welcome additions to the global health architecture and vital to the successful implementation of the Commission’s recommendations.
Oxygen is also an essential medicine for the management of many non-communicable diseases (NCDs) but especially for chronic respiratory diseases including chronic obstructive pulmonary disease (COPD), asthma, interstitial lung disease, and pneumoconiosis. These conditions affect 480 million people worldwide, including 96 million children under 15, and are responsible for more than 4 million deaths each year.
Concerned that the oxygen needs of this vast population are not being heard by governments and global health agencies, the Commission released a statement calling for their recognition in the Political Declaration from the High-level Meeting on NCDs that was held at the UN General Assembly on 25 September 2025. Alongside the statement, a powerful personal story from Alexander Mandl who depended on medical oxygen for many years prior to a successful double lung transplant, was shared.
Read and share the Statement here and Alexander’s story here!

**Don’t miss the full report of the Africa launch in Nigeria with Communique here!
Updates
Regional Launches
- Middle East and North Africa: International Primary Care Respiratory Group (IPCRG) World Conference, 11-14 June, 2026, Tunis, with Lancet Global Oxygen Commissioner, Professor Fatoumata Dicko Touré and Dr Valerian Leroy, Institut National de la Santé et de la Recherche Médicale (INSERM).

- Africa: Africa Primary Health Care Forum, 15 July, 2025, Abuja, with Lancet Global Health Oxygen Commissioner, Professor Adegoke Falade, Dr Carina King, Karolinska Institutet, Dr Francis Ohanyido, WAAPH, Chizoba Fashanu, Clinton Health Access Initiative, Dr Suleiman Saidu Bashir, Forum of State Primary Health Care Development Agencies, Dr Hadiza Khamofu, FHI 360, Cristian Munduate, UNICEF Nigeria, Aishat Adeniji, HealthPort and Africa Health Business Symposium, 16 July, 2025, with Noha El-Ghobashy, Oxygen Hub, Amarpreet Rai, Sanrai International, Aishat Adeniji, HealthPort, and Nnamdi Agbim, Interkel Nigeria Limited.

- Europe: INSPiRED, 27 June, 2025, Barcelona, with Lancet Global Health Editor-in-Chief, Zoë Mullan, Commissioner Professor Heather Zar, Dr Eric McCollum, Dr Carina King, Dr Catia Cillóniz (pictured) and Dr Karen Czischke, with special testimony from the family of 21-month-old baby Blai Perramon Castillo.

- South Asia: Regional World Health Summit, 27 April, 2025, New Delhi, with One Health Trust, WHO SEARO, PATH, National Neonatology Forum, Global Coalition of TB Advocates, and more.

- Western Pacific: Australian Global Health Alliance 2025 Congress, 2 April, 2025, Sydney, represented by lead Commission author Hamish Graham from the University of Melbourne and the Murdoch Children’s Research Institute below.

- North America: Consortium of Universities for Global Health (CUGH) Annual Conference, 20 February, 2025, Atlanta, represented by Oxygen Commissioner Shams Arifeen (below) and author Dr Ehsan Rahman from icddr,b.

Other events
- International Union Against Tuberculosis and Lung Disease, World Conference on Lung Health, Copenhagen, Denmark, 18-21 November, 2025 with the Union Child Pneumonia Working Group, co-chaired by Dr Carina King from Karolinska Institutet, Sweden, and Dr Rebecca Nantanda from Makerere Lung Institute, Uganda.
- Uganda Ministry of Health and Makerere University, National Annual Communicable and Non-communicable Diseases and 19th Joint Scientific Health Conference, Kampala, Uganda, 5 November, 2025 with Lancet Global Health Commissioner, Professor Freddie Ssengooba and author Dr Freddy Kitutu from Makerere University, Commissioner Rediet Shimeles Workneh from Ethiopia, and many more.
- World Society of Pediatric Infectious Diseases (WSPID), 14th World Congress, Bangkok, Thailand, 29 October, 2025, with Lancet Global Health Commission authors Dr Hamish Graham, Dr Ehsan Rahman, Leith Greenslade, representatives from the Health Ministry and Clinton Global Health Access Initiative (CHAI) in Lao PDR, and PATH in Viet Nam.

- icddr,b, Bangladesh Oxygen Summit, Dhaka, Bangladesh, 7 October 2025, with Lancet Global Health Oxygen Commissioner Dr Shams El Arifeen, lead author Dr Ehsan Rahman, and more.

- Alfred Emergency Academic Centre, Global Emergency and Critical Care Symposium, Melbourne, Australia, 10 September 2025, with Lancet Global Health Oxygen Commission lead author, Dr Hamish Graham.

- Council of International Neonatal Nurses COINN Zambia, 14-15 August, 2025 with Lancet Global Health Oxygen Commission lead author, Dr Hamish Graham and neonatal nurse Dires Birhanu from Ethiopia and the release of a new Commission Statement on the vital role of pulse oximetry and medical oxygen for newborn survival.

- Asian Development Bank (ADB) INSPIRE Health Forum, 7-11 July, 2025 with Lancet Global Health Oxygen Commission lead author, Dr Hamish Graham and representatives from the governments of Japan, Fiji, Cook Islands, and Armenia, and The Global Fund, Unitaid, World Health Organization South-East Asia, The Pandemic Fund, Resolve To Save Lives, and the ADB.

RESOURCES
One year later…
Read about progress since the publication of the Commission report in:
- From evidence to action: taking stock of the Lancet Global Health Commission on medical oxygen security after a year, published in May 2026 in The Lancet Global Health.
Reactions
Read what stakeholders are saying about the Commission and how they are advancing implementation of its recommendations:
- Global Oxygen Alliance (GO₂AL), March 2025
- Sanrai International, March 2025
- PATH, February 2025
- One Health Trust, February 2025
- Murdoch Children’s Research Institute (MCRI), February 2025
Media
- Why over 5 billion people still lack access to life-saving medical oxygen, News Medical Life Sciences, 23 February, 2025
- The global oxygen crisis, BBC Health Check, 20 February, 2025
- An Invisible Medical Shortage: Oxygen, New York Times, 18 February, 2025
- Stifled Oxygen Access, Global Health Now, 18 February, 2025
- Medical oxygen in short supply in many parts of world, The Hill, 18 February, 2025
- Report: Improving oxygen access, pandemic preparedness could save millions of lives, CIDRAP, 18 February, 2025
- Five billion people lack access to safe, affordable medical oxygen globally, Nigerian Tribune, 17 February, 2025
- 60% world population lacks access to medical oxygen, Vanguard Nigeria, 18 February, 2025
- A Global Oxygen Crisis Is Putting Millions of Lives at Risk, Science Alert, 19 February 2025
- 5 billion globally lack access to medical oxygen, poor nations most affected: Lancet report, The Economic Times, 18 February, 2025
- Post-Covid lessons not learnt: Lancet flags five billion people still lack access to medical oxygen, The Indian Express, 20 February, 2025
Statements
- Medical Oxygen and NCDs, United Nations General Assembly, 17 September 2025
- International Neonatal Nurses Day, 15 August, 2025
- Commissioner Call to Action for World Oxygen Day, 2 October 2024 (Spanish)
- Milestone Medical Oxygen Meeting an Opportunity for Countries to Make Rapid Progress on Access, 10 May 2024
- UN General Assembly Lancet Global Health Oxygen Commission Statement, 15 September 2023 (French) (Spanish)
- Milestone Adoption of Medical Oxygen Resolution & Launch of new Global Oxygen Alliance at the World Health Assembly, 26 May 2023
- WHO Oxygen Resolution a Major Milestone for Access to Medical Oxygen, Every Breath Counts, 3 February 2023
- Welcoming the Lancet Global Health Commission on Medical Oxygen Security, Every Breath Counts, 25 September 2022
- Announcing the Lancet Global Health Commission on Medical Oxygen Security, Lancet Global Health, 23 September 2022
Latest from the Commissioners, Advisors, and Executive Committee
- Lisa Smith (with Kimberly Green), Medical oxygen—a missing piece in the noncommunicable diseases agenda, PATH, September 2025
- Leith Greenslade, Expanding Medical Oxygen Access Without U.S. Foreign Aid, Think Global Health, March 2025
- David Lowrance, et al, A rapid facility-level assessment of oxygen systems in 39 low-income and middle-income countries: a cross-sectional study, Lancet Global Health, February 2025
- Adegoke Falade with Rami Subhi, Towards equity: the unfinished crisis of medical oxygen, Lancet Global Health, February 2025
- Ramanan Laxminarayan, Reducing global inequities in medical oxygen access: the Lancet Global Health Commission on medical oxygen security, One Health Trust, February 2025
- Lisa Smith, Report on medical oxygen finds a 70 percent coverage gap and calls for action to end suffering and death, PATH, February 2025
- Hamish Graham, Global action needed to solve the medical oxygen crisis, Murdoch Children’s Research Institute, February 2025
- Steve Howie with Sainimere Boladuadua, Widespread suffering and death from lack of medical oxygen, University of Auckland, February 2025
- Tim Baker, Lack of access to medical oxygen is causing widespread suffering and death, Essential Emergency and Critical Network, February 2025
- Hamish Graham, Putting Oxygen Access on the Global Health Agenda, Regional World Health Summit, May 2024
- Neelima Navuluri, Filling the Oxygen Gap. Patients in low-income countries often aren’t getting adequate medical oxygen, a new DGHI-led study reveals, February 2024, based on Prevalence and phenotypic trajectories of hypoxaemia among hospitalised adults in Kenya: a single-centre, prospective cohort study, BMJ Respiratory Medicine, September 2023
- Lisa Smith, et al, Variability of oxygen requirements in critically ill COVID-19 patients, Journal of Global Health, February 2024
- Shams el Arifeen, et al, Implementation of bubble continuous positive airway pressure for children with severe pneumonia and hypoxemia in intensive care unit of Dhaka Hospital, Bangladesh, Pediatric Pulmonology, January 2024
- Ramanan Laxminarayan with Varun Manhas, National Medical Oxygen Grid, October 2022, Overview Deck, and Letter of Support from Madhya Pradesh Government, January 2024
- Hamish Graham, Freddy Kitutu, Freddie Ssengooba, Felix Lam, et al, Improving Effective Coverage of Medical Oxygen Services For Neonates and Children in Health Facilities in Uganda: A Before-After Interventional Study, The Lancet Preprint, December 2023
- Tisugane Mvalo, Eric McCollum, et al, A hidden pandemic: the danger of donated respiratory devices to children in LMICs, Lancet Global Health, December 2023
- Heather Zar and Eric McCollum, Pulse oximetry to detect paediatric hypoxaemia-the fifth vital sign, Lancet Global Health, November 2023
- Ramanan Laxminarayan and Leith Greenslade, Solving for Oxygen, Think Global Health, September 2023
- Robert Matiru with Zachary Katz, Opinion: Adopting WHO’s oxygen resolution is imperative to save lives, Devex, March 2023
ARTICLES

Historic Milestone: 71% of World’s Children Protected Against Pneumococcal Disease
Statement by the Secure PCV Collaborators in response to the WHO/UNICEF Estimates of National Immunization Coverage (WUENIC) More than seven in every ten infants are protected with three doses of the pneumococcal conjugate vaccine (PCV) in 2025, according to the latest vaccine coverage estimates from...
27 July, 2026
Childhood Pneumonia Takes Center Stage at INSPiRED 2026
The 4th Congress of the International Society of Pediatric Respiratory Diseases (INSPiRED), held in Bologna in June 2026, demonstrated that we have entered a new era of pneumonia control, where rapid reductions in child mortality are within reach. Across the Congress, presentations highlighted advances in...
07 July, 2026
Financing Maternal RSV Immunization Through Reduced-Dose PCV Schedules
Pneumonia remains the leading infectious cause of death among children under five, accounting for more than 600,000 deaths annually worldwide. Despite gains in vaccine coverage, progress reducing pneumonia deaths has slowed, and many countries face increasingly constrained health budgets. At the same time, new tools...
05 June, 2026
The power of civil society to support new vaccine introductions
Something extraordinary has been happening for the children of Chad, Somalia, and South Sudan. An unprecedented period of child health progress with the introduction of new vaccines against pneumonia, diarrhea, and malaria. Together, these three infections caused 86,000 deaths in 2021 – 45% of all...
22 June, 2025
Best Practices for Pulse Oximeter Use!
“Functional, good-quality pulse oximeters should be available in every area where patients are clinically assessed or admitted in sufficient quantities to meet all needs,” The Lancet Global Health Commission on Medical Oxygen Security Do you want to improve the use of pulse oximetry among children...
06 June, 2025
Climate change and respiratory health
Climate Change and Respiratory Health, brought together four leading experts – Heather Adair-Rohani from the World Health Organization (WHO), Rebecca Nantanda from Makerere University Lung Institute, Laura-Jane Smith from the British Thoracic Society, and John Sampson from Johns Hopkins University to explore different facets of...
11 December, 2024